The latest news, analysis and opinion ✓ NEWS of the WORLD incorporates The Invisible Man XaX ✓ For back posts, see http://cyberianz.blogspot.com and https://invisiblepaul.blogspot.com ✓ The editor does not necessarily agree with opinions expressed on this site, though often he does.
Where the Spirit of the Lord is, there is liberty.
The Petersens bless us with this John Denver classic. Katie brings to this fine rendition her usual amazing vocals and instrumentalism. (She calls her special five-string fiddle "Moses." No idea why... )
Backup link https://youtu.be/hhosbEuhl6I?list=RDhhosbEuhl6I
In a joint open letter, The Times, The Guardian, Le Monde, Der Spiegel and El País said the prosecution of Mr. Assange under the Espionage Act “sets a dangerous precedent” that threatened to undermine the First Amendment and the freedom of the press.
NOVEMBER 28, 2022
An Open Letter from Editors and Publishers: Publishing is Not a Crime
The U.S. government should end its prosecution of Julian Assange for publishing secrets.
Twelve years ago, on November 28th 2010, our five international media outlets – the
ork Times, the Guardian, Le Monde, El Pais and Der Spiegel – published a series of revelations in cooperation with Wikileaks that made the headlines around the globe.
“Cable gate,” a set of 251,000 confidential cables from the US State Department disclosed corruption, diplomatic scandals and spy affairs on an international scale.
In the words of the
York Times, the documents told “the unvarnished story of how the government makes its biggest decisions, the decisions that cost the country most heavily in lives and money.” Even now in 2022, journalists and historians continue to publish new revelations, using the unique trove of documents.
For Julian Assange, publisher of Wikileaks, the publication of “Cable gate” and several other related leaks had the most severe consequences. On April 11th, 2019, Assange was arrested in London on a US arrest warrant, and has now been held for three and a half years in a high security British prison usually used for terrorists and members of organized crime groups. He faces extradition to the US and a sentence of up to 175 years in an American maximum security prison.
This group of editors and publishers, all of whom had worked with Assange, felt the need to publicly criticize his conduct in 2011 when unredacted copies of the cables were released, and some of us are concerned about the allegations in the indictment that he attempted to aid in computer intrusion of a classified database. But we come together now to express our grave concerns about the continued prosecution of Julian Assange for obtaining and publishing classified materials.
The Obama-Biden Administration, in office during the Wikileaks publication in 2010, refrained from indicting Assange, explaining that they would have had to indict journalists from major news outlets too. Their position placed a premium on press freedom, despite its uncomfortable consequences. Under Donald Trump however, the position changed. The DOJ relied on an old law, the Espionage Act of 1917 (designed to prosecute potential spies during World War 1), which has never been used to prosecute a publisher or broadcaster.
This indictment sets a dangerous precedent, and threatens to undermine America’s First Amendment and the freedom of the press.
Holding governments accountable is part of the core mission of a free press in a democracy.
Obtaining and disclosing sensitive information when necessary in the public interest is a core part of the daily work of journalists. If that work is criminalised, our public discourse and our democracies are made significantly weaker.
Twelve years after the publication of “Cable gate,” it is time for the U.S. government to end its prosecution of Julian Assange for publishing secrets.
A climate scientist who left her academic ivory tower to tackle climate "alarmism" insists that there is no global warming emergency but that, even if there were, there isn't much to be done about it now.
In a wide-ranging 35-minute interview with BizNewsTV [https:biznews.com], Judith A. Curry, who as a professor specialized in extreme weather events, argues that too fast a transition from fossil to renewable energy is far more dangerous to humanity than any risk of human-induced global warming or global climate change, which she sees as slight.
Yet the warming that the earth is experiencing, aside from being within normal bounds, is on the whole better for people than not, the scientist says. [Story continues below.]
Now as a consultant to federal agencies, insurance companies and energy companies, Curry brings her extensive background to bear on the climate debate, challenging "manufactured consensus," some scientists who "exaggerate" climate issues and a movement of UN-linked socialists who, she says, are using climate fears as a wedge issue -- even to the point of generating very bad psychological effects among the world's children.
Yet, she insists, there is little if any scientific evidence to support the claims of the "doom and gloom" crowd. Yes, Curry says, there is no dispute that global warming has been happening, and there is legitimate, honest disagreement among scientists as to the causes. From her perspective however Mother Nature is the prime mover of climate, which has always been variable. Shifts in the sun's radiation, volcanic events and ocean warming and current oscillations are among the biggest factors. She regards carbon from fossil fuels as having only a "miniscule" effect on climate, but even if the effect were quite large, the "climate is going to do what it is going to do" and ideas for climate modification are fantasies.
Curry, when she was chairwoman of the School of Earth and Atmospheric Sciences at the Georgia Institute of Technology, focused her research on hurricanes, remote sensing, atmospheric modeling, polar climates, air-sea interactions, climate models, and the use of unmanned aerial vehicles for atmospheric research. She was a member of the National Research Council's Climate Research Committee, published more than a hundred scientific papers, and co-edited several major works. Curry left academia in 2017.
Curry argues that developed nations have done very well from fossil fuels, while undeveloped nations pay harsh penalties for being denied access to them by "the powers that be" behind international lending programs. She cites Bangla Desh as a place that, under good political leadership, avoided fossil fuel extremism and went from being an international "basket case" to a thriving nation. Because immediate survival concerns have been alleviated by a superior energy supply and rational economics, the nation's birth rate has plummeted from fantastically high to a rate comparable to those of developed nations, she says. [That is, poor people no longer feel the need to have plenty of children to counter high childhood mortality and for other poverty-tied reasons.]
Curry says that warming in the United States of the 1930s was worse than it is now, with extremes of forest fires, droughts and floods. But the warming trend has been mainly tracked from the 1970s, meaning there is little realization that the trend signals nothing unusual.
Curry notes that the alarmists have gone from focusing on warming to extreme weather events because of "trying to figure out how to get attention." Warming isn't nearly so compelling as big floods and hurricanes, she asserts. There may be a "minimal component from global warming" in extreme weather events "but it's very difficult to tease out from natural variability." There is "no objective way" to determine the validity of such a claim. [When your local weather person reports that yesterday broke a temperature record, this does not necessarily imply anything unusual. No specific day is likely to hit the average on the nose; there is always statistical variation around the mean or average.]
She blames some of the concern about such extremes as a consequence of a hyper-wired world of internet communications.
The 63-year-old argues that "people's world views, their politics, career investments" are behind what she sees as unsupportable claims. In particular, academics are under great pressure to conform to the carbon-emissions line or face losses of grants and career sidelining. [Even private universities are highly dependent on federal science grants. Organizations such as the colossal Blackrock investment fund have used their extensive influence in business, finance, media and politics to promote what Blackrock chief Laurence D. Fink sees as a world-saving green agenda.]
The former educator asserts that the Greta Thunberg phenomenon has had a devastating impact on the world's children, who lack the critical thinking filters needed to assess doom talk. "It's very hard to counter this," with the result that depression and suicidal thinking among children are on the increase. She fears that the world won't generate enough engineers and other professionals as children lose heart in educational attainment (tho she spoke only generally on this point, not citing any research).
The scientist argues that a rushed transition from fossil fuel to non-fossil energy will actually "take a lot of fossil fuel" in terms of mines and manufacturing. While the goal of non-fossil fuels may be laudable, an extreme approach can only make matters much worse, she says. The suffering caused by lack of access to energy is much higher on the scale than any suffering likely to come from additional CO2 in the atmosphere, she asserts. In general, modern humans in energy-consuming lands are much better off than their forebears, she says.
The scientist argues that the goal of "net zero" emissions is of dubious value, arguing that "we will cycle out" of the current warming trend within five or 10 years, as happened innumerable times in the past. "Even if we went to net zero, we would still have extreme weather events." [Net zero refers to the balance between the amount of greenhouse gas produced and the amount removed from the atmosphere. We reach net zero when the amount we add is no more than the amount taken.]
She points out that northern hemisphere weather at the end of pre-industrial times wasn't ideal. The world was coming out of the Little Ice Age, she says, with consequent problems of crop failure and famine.
As long as disastrously hasty energy transitions are avoided, by the end of this century "we are all going to be better off -- even with some minor environmental damage from warming," she insists. Decades are required for development of ultra-clean renewables, she argues. That point needs to be borne in mind by policymakers, the scientist says.
The biggest consequence of warming is rise in sea level. As projections put this at inches per year, it is something humans can deal with. Only if there were a sudden collapse of the arctic ice sheet would global catastrophe ensue, she says, asserting that such an event is more likely to come in response to some undersea volcanic-seismic event.
Those who see "the earth as fragile" and in peril from carbon emissions hold a "world view that doesn't align with reality."
Curry says that the climate change agenda goes back to a UN treaty in 1992, before there was any sign of global warming. The United States had just been coming out of a decades-long cooling trend, she observed.
This must be the product of a great conspiracy, a conspiracy on a scale so immense as to dwarf any previous such venture in the history of man. A conspiracy of infamy so black that, when it is finally exposed, its principals shall be forever deserving of the maledictions of all honest men.
It's true that we don't yet know how Twitter chief Elon Musk plans to implement his plan to limit the reach of those whom he feels go too far in their tweets. But, notice that the giant multinational corporations aren't waiting to find out. They clearly prefer a system with a very narrow bandwidth for acceptable talk, a system they control via legacy media and big tech. That system benefits a very small group of powerful people -- the globalist elite -- who wish to protect their positions by holding power to keep Americans and all others unaware of their doings and agendas.
Rest assured that the conspiracy that is gunning for Musk is the same cabal that is pressing to have Wikileaks founder Julian Assange brought to the United States and tried for breaking their monopolistic control of information. Would you not think the U.S. press would be highly concerned about the Justice Department's transparent ruse to set a precedent for limiting freedom of speech?
You would be wrong if that's what you thought. The legacy media are NOT INTERESTED in the first amendment. They are interested in protecting their conspiratorial masters -- many of whom are up to their armpits in greedy guts schemes to feed at communist China's trough.
For intriguing and often moving listening and visual experiences, you can do no better than
Paige Anderson and the Fearless Kin, a marvelous youth band from northern California. The members are all grown and gone separate ways now, but their videos are still quite something.
Dr Sanjay Verma says data show that the more covid vaccine that is taken, the more the probability of myocarditis -- especially among male teenagers.
In the interview below, the CDC practice of limiting the data it publishes is called into question.
Verma, the author of a statistical vax data study, says other cardiologists around the nation would speak to him of enormous surges in cases of myocarditis -- or, heart inflammation -- that occurred after mass vaccination began.
Tho the CDC says (see previous post) that its VAERS data -- on adverse health effects after vaccination -- cannot alone be relied on, Verma says that the agency in its published work takes no account of other databases, such as those for health insurance, leading to unrealistically low risk assessments for covid vaccines.
Yet, he says, the CDC has found an increased risk of post-vaccine arrythmia (where the heart beats erratically) among monitored heart patients -- particularly those with inflammation.
The CDC has failed to clearly warn vaxxed myocarditis patients to strictly avoid strenuous aerobic physical activity for three to six months after the ailment is detected because of heightened risk of sudden collapse and death.
The doctor charges that on social media physicians who don't choose their words with great care are censored if they link covid vaccines to sudden adult death syndrome. He argues that since the vax rollout such deaths have skyrocketed, tho others say the increase cannot be definitively linked to vaccines. (For example, fentanyl has caused major increases tho such deaths are generally easily diagnosed.)
Verma however cautioned that during covid lockdowns some increase in VAERS data may have been due to heightened concern of smartphone-wielding citizens. Anyone can file a VAERS report.
Verma says a "good question" is why the CDC's website still uses early vaccine efficacy data -- which show very high effectiveness -- rather than data from subsequent studies, which show dramatic drop-offs in effectiveness among the populace.
Sees network of criminal, satanic forces in bid to take over world.
We must fight wicked conspiracy, whistleblowing archbishop insists. Viganò's strong warning https://rumble.com/v1w4jom-archbishop-carlo-maria-vigano.html
(Video from Charles Kovess, an Australian commentator.)
Archbishop Carlo Maria Viganò
As a high Vatican official, Archbishop Carlo Maria Viganò blew the whistle on a Vatican financial scandal and on a U.S. archbishop's pedophile scandal.
When I tried this link directly from my Blogspot blog, it failed. But when I cut it and pasted it into the browser bar, it worked. (Good luck!)
Those who read that Wikipedia page are, it seems, being tracked by someone. In the URL above, the final six characters are added only after one tries to reach the page from a Google search item. But if one cuts and pastes the URL that was originally in place (from which the final "o" is clipped in the altered link above), one is sent to a Wikipedia dead-end page.
Just in case you might be interested, I am sending along links to two other of my blogs, along with links to two of my e-books. (If a link fails, try cutting and pasting it into your browser bar.)
blog is highly personal. There you're likely to find a lot of stuff about my favorite group, the Petersens.
Notes on Notes includes the disclaimer:
What's up with this "blog"?
This "blog" is meant more as a message board than a blog. I post many quickie ideas for a few people to take or leave. Other random viewers may be perplexed that so many posts are taken down after only hours or days. Well, the stuff isn't meant for anything more than a quick heads up, or a "that's real cool," or a "what about this (probably zany) idea?" I also post all kinds of music videos -- just 'cauz. This way, I needn't fill up certain inboxes with a bunch of unsolicited stuff. In any case, great words of wisdom are definitely not what this message board is about
For the word of God is quick, and powerful, and sharper than any twoedged sword, piercing even to the dividing asunder of soul and spirit, and of the joints and marrow, and is a discerner of the thoughts and intents of the heart. -- Hebrews 4:12
The New York Times used to say that the Hunter Biden laptop matter was "bogus" and a "hoax."
Now not so.
But it still says the Sandy Hook "non-massacre" data are part of a "hoax" and are "bogus."
Would the Times help us understand who put out a doctored, distorted photo of Adam Lanza, the purported killer, that made him appear to be wildly abnormal? Who went on the internet to slap up that bogus, hoax photo used by media worldwide? And why was it done?
The doctored photo below is attributed to NBC News.
The next photo, also attributed to NBC, is slightly more credible, tho one can be forgiven for suspecting that the bug eyes were added in order to make the kid look as crazy as possible.
The government's vaccine safety data that show deaths following covid vaccination cannot, for scientific reasons, be trusted by the public, a top CDC official asserts.
Dr. Michael McNeil was responding to a physician's query about a study based on government data in its Vaccine Adverse Event Reporting System (VAERS) that showed a surge in deaths following vaccination for covid. McNeil is acting director of the Immunization Safety Office at the Centers for Disease Control and Prevention (CDC).
As "CDC was not involved with the work you mentioned in your correspondence, which used limited information from a publicly accessible VAERS database," the agency is, McNeil wrote,
"unable to comment on this analysis conducted outside of the agency."
Even so, McNeil implied that the study was no good by saying, "Statements that imply that reports of deaths to VAERS following vaccination equate to deaths caused by vaccination are scientifically inaccurate, misleading, and irresponsible."
A problem with the government's public databank is that healthcare providers must report deaths after vaccination even if they don't think vaccination was the cause, McNeil said. Also, he said, only 10 percent of VAERS reports are of a serious nature -- tho that fact would seem to have little to do with the matter at hand: the serious reports.
Around 90% of reports to VAERS after COVID-19 vaccination have been non-serious. Healthcare providers who administer COVID-19 vaccines are required under the provider agreements for the CDC COVID-19 Vaccination Program and Emergency Use Authorizations (EUAs) by the Food and Drug Administration (FDA) to report certain serious adverse events, like deaths, to VAERS regardless of whether the reporter thinks the vaccine caused the adverse event. This required reporting is one reason why many reports to VAERS do not represent adverse events caused by the vaccine.
McNeil does not discuss statistical methods used by his office that might tend to rule out correlation by random chance nor does he say categorically that the CDC has never detected anything more than weak correlations between covid vaccine and deaths.
He cites a CDC statement that more than the VAERS databank are used to detect vaccine "safety signals" and seems to suggest that the CDC's experts are the only ones competent to analyze vaccine safety data.
McNeil writes,
CDC has been publicly presenting and openly discussing data from our vaccine safety monitoring systems regarding coronavirus disease 2019 (COVID-19) vaccinations at meetings of the Advisory Committee on Immunization Practices (ACIP) and we have also regularly published analyses of these data. Statements that imply that reports of deaths to VAERS following vaccination equate to deaths caused by vaccination are scientifically inaccurate, misleading, and irresponsible. We continue to monitor these and other adverse events using our safety surveillance systems.
The CDC statement asserts,
The strengths of VAERS are that it is national in scope and can often quickly detect an early hint or warning of a safety problem with a vaccine. VAERS is one component of CDC's and FDA's multifaceted approach to monitoring safety after vaccines are licensed or authorized for use. There are multiple, complementary systems that CDC and FDA use to capture and validate data from different sources. VAERS is designed to rapidly detect unusual or unexpected patterns of adverse events, also referred to as "safety signals." If a possible safety signal is found in VAERS, further analysis is performed with other safety systems, such as the CDC’s Vaccine Safety Datalink (VSD) and Clinical Immunization Safety Assessment (CISA) Project, or in the FDA BEST (Biologics Effectiveness and Safety) system. These systems are less impacted by the limitations of spontaneous and voluntary reporting in VAERS and can better assess possible links between vaccination and adverse events. Additionally, CDC and FDA cannot provide individual medical advice regarding any report to VAERS.
No one is running away at this time, say officials as military bind tightens
Tho Russia's Crimean front-men are denying reports that a city on the Crimean neck is being evacuated, Ukraine resistance forces point to a move to shift a Russian military corridor out of that city, which is now within range of Ukrainian missiles and drones.
The reports of evacuation have not been confirmed, but a possible Russian move to shift a military corridor out of Armyansk in the northern Crimean neck would appear to make sound sense militarily.
From the Institute for the Study of War:
Crimean occupation officials demonstrated heightened unease on Nov. 22, likely over Ukrainian strikes on Russian [ground lines of communication] on the peninsula and ongoing military operations on the Kinburn Spit. Russian sources shared footage of Russian air defenses activating on Nov. 22, claiming that Russian forces shot down multiple Ukrainian drones over Crimea.
Crimea occupation head Sergey Aksyonov subsequently announced that Crimea is raising its terrorist threat level to high (yellow) until at least Dec.7.
Russian [militarist bloggers] claimed that Russian authorities are preparing for an evacuation of administration officials and military equipment in Armyansk (about 100 km southeast of Kherson City) due to the threat of Ukrainian strikes on northern Crimea.
A milblogger even claimed that he helped conduct the evacuation, while another milblogger claimed that women and children are already evacuating from Armyansk.
Aksyonov denied evacuation claims, and some milbloggers claimed that Armyansk occupation authorities conducted evacuation exercises.
ISW is unable to confirm the veracity of these claims.
The Ukrainian Resistance Center also reported that Russian forces are planning to expand a road on the Arabat Spit (45 km from Dzhankoy) to transfer military equipment in an effort to relocate the [military corridor] from Armyansk.
ISW assesses that Ukrainian forces are unable to conduct an immediate attack on Armyansk, but these claims likely indicate that Russian authorities are exhibiting a level of worry close to panic.
Crimea evac reports termed 'fake news' https://ua.krymr.com/a/news-krym-feiky-evakuatsia-armiansk/32142649.html
British doctors and other experts have published the following open letter warning of dangers in giving covid vaccines to pregnant women.Obstetricians and gynaecologists in the U.K. have put their faith in and adjusted their practice according to guidance from their Royal College (RCOG). However, recent advice from the RCOG has been in complete contradiction to everything that it itself and academic institutions have been teaching about evidence-based medicine. This advice is that: COVID-19 vaccines are not only safe but strongly recommended for pregnant women.
Such advice is not grounded in robust data based on ethically conducted research – and anyone who is medically and academically trained should take serious issue with this.
Ethics of clinical research
Clinical researchers, especially when conducting trials to investigate pharmaceutical products, are required to update themselves every two years on the principles of Good Clinical Practice, which incorporate the Nuremberg Code and the Declaration of Helsinki. According to those principles, it is unethical to violate a study protocol by under-reporting adverse events, by removing subjects with adverse events from the study and by unblinding study participants prematurely with the purpose of administering the product under investigation to everyone and therefore effectively ending the trial – as have all happened in the COVID-19 vaccine trials. It is unethical to prevent the public from accessing raw trial data for 75 years and to only release some of it for independent scrutiny after a lawsuit. It is unethical to extrapolate the conclusions of a prematurely ended trial to vulnerable groups not represented in the trial – such as pregnant women.
For obvious reasons, pregnant women are usually excluded from clinical trials. The British National Formulary frequently advises against the use of a pharmaceutical product in pregnancy as a precaution due to lack of data. In pregnancy, lack of data is sufficient to be hesitant. Two examples in the not-too- distant past remind us how disastrously wrong it can go when a new product is given to pregnant women: thalidomide caused severe limb defects in the foetus, and diethylstilbestrol (DES) increased the risk of certain cancers after exposure in utero, requiring life-long surveillance for more than one generation. It was indeed the thalidomide scandal which led to the establishment of the U.K. Yellow Card system for adverse event reporting. But suddenly all of this seems to be forgotten.
Lack of robust and reliable safety data
A recent public controversy focused on MHRA advice updated on August 16th 2022 stating in the toxicity conclusions that “sufficient reassurance of safe use of the vaccine (mRNA BNT162b2/Pfizer/BioNTech) cannot be provided at the present time” and “women who are breastfeeding should also not be vaccinated”. The Government and the RCOG were very quick to express their concerns about the circulation of this apparent misinformation and to reinforce their advice that pregnant women should get vaccinated. This document was originally from December 2020, and so the claim is that this section is outdated. The question remains why this section was not amended if this document was recently updated. The answer is of course because there is nothing to update it with: studies regarding genotoxicity, carcinogenicity, reproductive and developmental toxicity, and prenatal and postnatal development have still not been conducted.
It cannot possibly be known whether it is safe to give these products to pregnant and breastfeeding women. Clinical research standards dictate close and prolonged observation of trial subjects, documenting any and all observed clinical effects following administration of the trial compound. This has not been done. There are no trials that last even the duration of a pregnancy. COVID-19 vaccines were on the market for a mere four months when the initial advice to avoid them in pregnancy changed by 180 degrees and they were declared safe. Potential adverse effects for the offspring have not even been considered.
It is profoundly unethical to give a completely novel compound to pregnant women on a mass scale without the strict protocols of clinical research to just see what happens and then pretend that this is science. Yet this is exactly what has been happening.
Incorrect interpretation of available data
Safety data are largely based on retrospective and observational cohort analyses and registries, such as the CDC’s V-Safe COVID-19 Vaccine Pregnancy Registry. Voluntary registries are not equivalent to well-designed prospective clinical trials, as follow-up is inconsistent and incomplete with no standardisation or systematisation and no tracking of participants.
Other data are from short-term studies where outcomes are determined in post hoc analyses, with little or no stratification of gestational age at the time of vaccination. A large Canadian study published in the Lancet concluded that “COVID-19 vaccines have a good safety profile in pregnancy” based on a follow-up period of a whole seven days. Conflicts of interest status on this paper is notable. Publications are clearly biased towards reaching the conclusions of affirming safety and effectiveness of COVID-19 vaccines in pregnancy even when their study data do not allow such conclusions. The U.K. Medical Freedom Alliance (UKMFA) has published on its website open letters to the U.K.-based authors of twosuch studies with a critique of their conclusions. Both papers were widely propagated to the public.
The systematic review and meta-analysis of the effectiveness and perinatal outcomes of COVID-19 vaccination in pregnancy was co-authored by the current president of the RCOG, who shared this headline with the RCOG membership: “COVID-19 vaccination associated with 15% reduction in stillbirths in pregnant women.” The prompt within the message to “Find out more” linked not to the original paper for everyone to scrutinise and recognise the flawed methodology, but to the Guardian propagating the same headline. The work of Professor Norman Fenton (Professor of Risk Information Management) on the “statistical illusion of better pregnancy outcomes for vaccinated women” is worth considering for a comprehensive analysis of the available data.
Currently, any quantitative assessment of the risks of adverse events in pregnancy is mostly stymied by the lack of reliable denominators, prohibiting accurate interpretation of existing data.
Shimabukuro et al. published their preliminary findings of mRNA COVID-19 vaccine safety in pregnancy in the NEJM based on the V-Safe registry, reporting a miscarriage rate of 12.6% – consistent with the general population. This was based on a denominator of 827 completed pregnancies. The conclusion was incorrect as only 127 women had been vaccinated in the first or second trimester, and so by definition the remaining 700 women could not possibly have had an early pregnancy loss.
According to post-marketing data from Pfizer, 42,086 adverse events were reported to the manufacturer during the first three months of the vaccination programme. Amongst these were reports from 270 pregnant women. Only 32 pregnancy outcomes were recorded. This should have been but indeed was not a study with dedicated follow-up. These data were collected as part of post-marketing surveillance and are insufficient for comprehensive analysis.
Therefore, there are no reliable statistics at this time – but there are plausible mechanisms of potential harm and there are glaring safety signals.
Mechanisms of potential harm
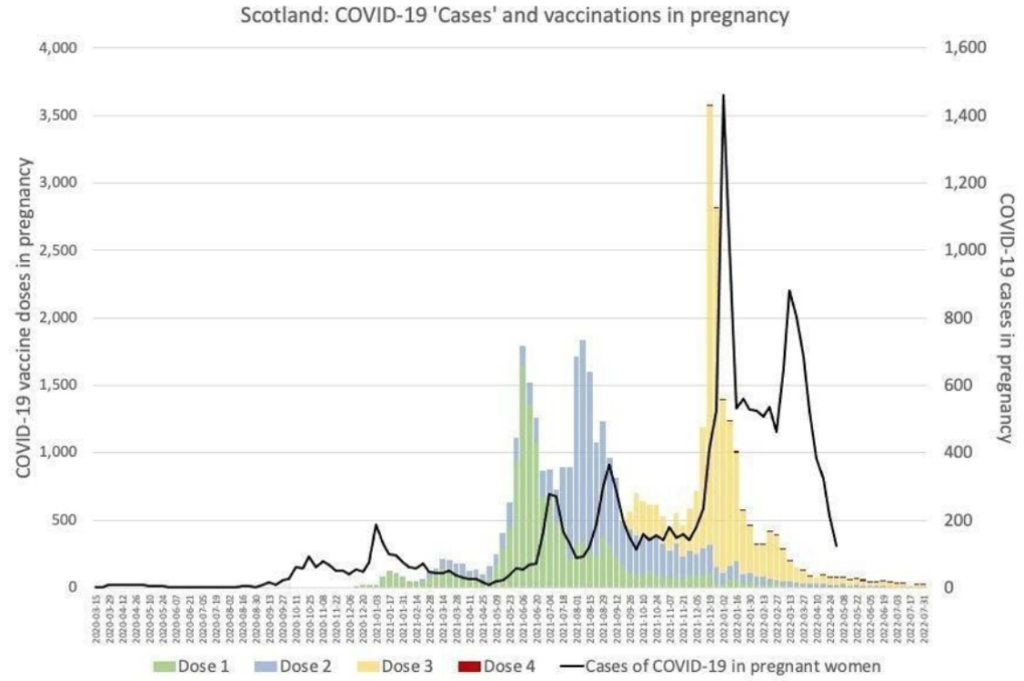
Even if pregnant women were at increased risk from COVID-19, there are no conclusive data demonstrating that those risks are mitigated by vaccination. Regarding effectiveness, it is worth considering the data tracking COVID-19 vaccination and infection in pregnancy in Scotland, which do not indicate vaccination to have been beneficial, indeed they suggest quite the opposite (Figure 1).
Figure 1
Independent of the potential risks to the pregnancy itself, there are now well-acknowledged risks of COVID-19 vaccines for women of childbearing age in general, including risks of cardiac and cardiovascular morbidities, which may well affect a pregnancy.
Pfizer’s own pharmacokinetics studies showed that the lipid nanoparticles used to carry the mRNA are distributed to and accumulate in the ovaries at significant concentrations (Table 1).
Table 1
A recent research letter in JAMA Pediatrics highlighted that COVID-19 vaccine mRNA could be detected in breast milk. The clinical significance of this has not been investigated, but the conclusion advises caution against breastfeeding for the first 48 hours after vaccination, and previous studies have described adverse events in 7.1% of breastfed infants.
A study published in PLOS Pathogens showed that in mice “the mRNA-LNP vaccine platform induces long-term immunological changes, some of which can be inherited by the offspring”. The effect on the immune system in human offspring – including defence against infections as well as the propensity to allergies and autoimmune disorders – is at this stage completely unknown.
Concern regarding potential autoimmunity is also based on molecular mimicry. mRNA vaccines induce human cells to produce antigens (spike proteins) in order to elicit an immune response. Similarities between spike protein and human proteins may lead to an adverse autoimmune reaction. It is potentially relevant for pregnant women that the SARS-CoV-2 spike glycoprotein was found to share similarities with 27 human proteins that relate to oogenesis, uterine receptivity, decidualisation and placentation in a study published in the American Journal of Reproductive Immunology.
Safety Signals
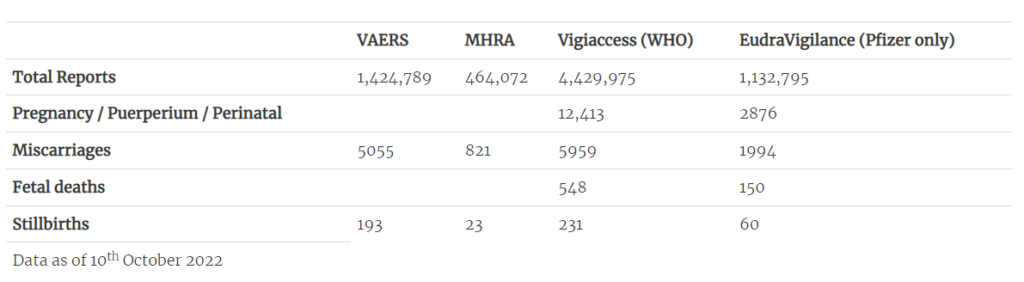
Most concerning are the accumulating safety signals – and the apparent reluctance to fully investigate them. All four major databases for adverse event reporting (VAERS, MHRA Yellow Cards, EudraVigilance, WHO Vigiaccess) contain significant numbers of pregnancy-related adverse outcomes, including miscarriages and stillbirths (Table 2).
Table 2: Pregnancy-related adverse events on international databases
A study – currently in preprint – by Dr. James Thorp (U.S. specialist in foeto-maternal medicine) compares pregnancy-related adverse outcomes reported after COVID-19 vaccination to those reported after influenza vaccinations. Even considering the limitations of the study and the perhaps questionable validity of this comparison, the number of reports following COVID-19 vaccines of miscarriages, foetal chromosomal abnormalities, foetal malformation, foetal cystic hygroma, foetal cardiac disorders, foetal arrhythmia, foetal cardiac arrest, foetal vascular mal-perfusion, foetal growth abnormalities, foetal abnormal surveillance, foetal placental thrombosis, low amniotic fluid and foetal death and stillbirth are extremely concerning.
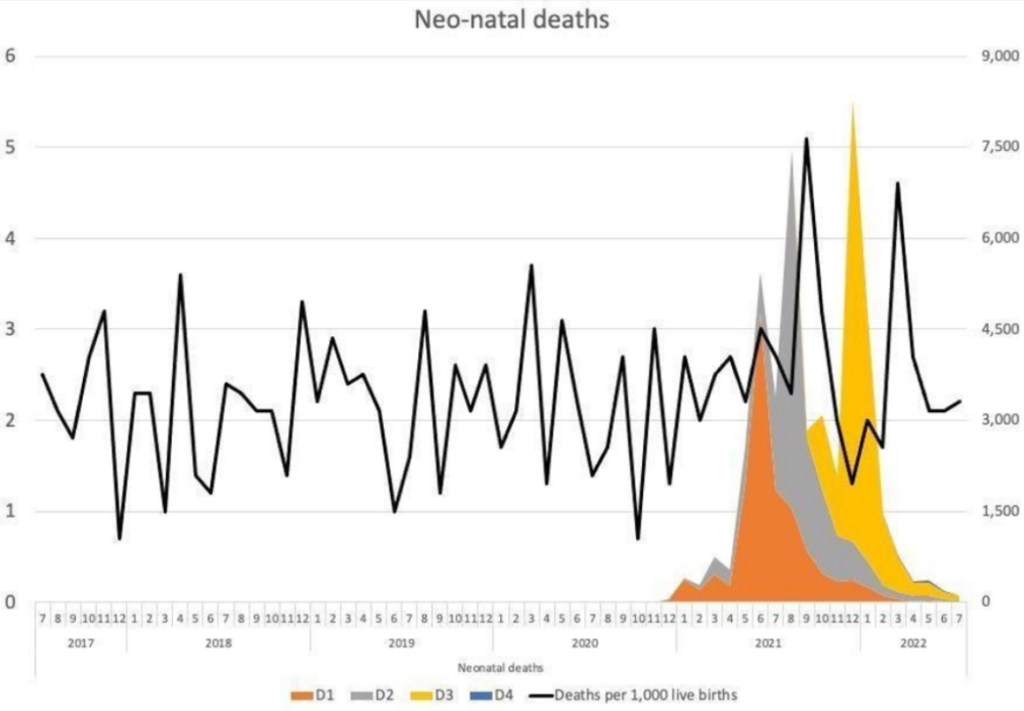
In addition, there are reports of unexplained phenomena. Birth rates in the first half of 2022 appear to have fallen significantly in highly vaccinated countries in Europe based on official figures, with a decline of more than 4% in 15 countries and more than 10% in seven countries. The rates of cumulative annualised infant mortality in Scotland show 2021 as a significant outlier (Figure 2). As the data are cumulative, the variation usually evens out towards the end of the year, but not so in 2021. The rise mostly relates to spikes in neonatal deaths, which have occurred in temporal association with COVID-19 vaccination (Figure 3). This correlation is especially remarkable considering not all pregnant women were vaccinated.
Figure 2: Infant mortality in Scotland 2015-2022
Figure 3: Neonatal deaths and COVID-19 vaccination (Dose 1-3) in pregnancy in Scotland
These spikes in neonatal deaths have been publicly acknowledged as concerning. Dr. Sarah Stock, expert in maternal and foetal medicine at the University of Edinburgh, commented in May 2022: “The numbers are really troubling, and I don’t think we know the reasons why yet”, but “stressed the Covid vaccine, which studies have consistently shown to be safe in pregnancy, was not a factor”. This cannot possibly be known unless it is investigated without the bias that has afflicted most publications on this subject to date. The need for investigation is urgent, and whilst this should have been with clinical trials, there should now be a moratorium on COVID-19 vaccines to allow for meticulous retrospective analysis and re-evaluation.
If we continue to ignore these safety signals, we are not doing our due diligence to protect patients from harm. According to the principles of Good Medical Practice outlined by the General Medical Council, we are supposed to take action when we are concerned about compromised patient safety.
We are not just concerned but deeply disturbed and alarmed at the widespread distortion of science and the blatant omissions in the process of bringing a newly developed pharmaceutical product to market.
We have a collective duty to restore the principles of medical ethics to our practice and to clinical research to protect the most vulnerable groups from harm, and this includes pregnant women and their babies.
In the absence of data on long-term outcomes of mRNA COVID-19 vaccination in pregnancy for either women or their infants, vaccination of pregnant women should be paused while a full safety enquiry is conducted and until results of long-term studies on animals as well as pregnant women and their offspring firmly and unequivocally establish that the benefits of vaccination clearly outweigh the risks to both mothers and babies.
We look forward to an early response to our concerns.
Dr Julia Wilkens, FRCOG, MD, Consultant in Obstetrics & Gynaecology
Dr John Williams, FRCOG, retired Consultant in Obstetrics & Gynaecology
Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMed Sci, Principal, Institute for Cancer Vaccines & Immunotherapy (ICVI)
Professor Richard Ennos, MA, PhD, Honorary Professorial Fellow, University of Edinburgh
Professor John Fairclough, FRCS, FFSEM, retired Honorary Consultant Surgeon
Professor Dennis McGonagle, PhD, FRCPI, Consultant Rheumatologist, University of Leeds
Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Honorary Professor of Professional Practice, Buckingham University
Lord Moonie, MBChB, MRCPsych, MFCM, MSc, retired member of the House of Lords, former parliamentary under-secretary of state 2001-2003, former Consultant in Public Health Medicine
Dr Victoria Anderson, MBChB, MRCGP, MRCPCH, DRCOG, General Practitioner
Julie Annakin, RN, Immunisation Specialist Nurse
Helen Auburn, Dip ION MBANT NTCC CNHC RNT, registered Nutritional Therapist
Dr David Bell, MBBS, PhD, FRCP(UK), Public Health Physician
Dr Mark A Bell, MBChB, MRCP(UK), FRCEM, Consultant in Emergency Medicine
Dr Michael D Bell, MBChB, MRCGP, retired General Practitioner
Dr Alan Black, MBBS, MSc, DipPharmMed, retired Pharmaceutical Physician
Dr Gillian Breese, BSc, MB ChB, DFFP, DTM&H, General Practitioner
Dr H Burger, MRCGP, DRCOG, General Practitioner
Dr David Cartland, MBChB, BMedSci, General Practitioner
Caroline Cartledge, RM, BA (hons), Midwife
Angela Chamberlain, BSc (hons), Midwife
Dr Peter Chan, BM, MRCS, MRCGP, NLP, General Practitioner, Functional Medicine Practitioner
Michael Cockayne, MSc, PGDip, SCPHNOH, BA, RN, Occupational Health Practitioner
James Cook, NHS Registered Nurse, Bachelor of Nursing (Hons), Master of Public Health (MPH)
Dr Clare Craig, BMBCh, FRCPath, Pathologist
Dr David Critchley, BSc, PhD in Pharmacology, 32 years’ experience in Pharmaceutical R&D
Dr Sue de Lacy, MBBS, MRCGP, AFMCP, UK Integrative Medicine Doctor
Dr Jayne LM Donegan, MBBS, DRCOG, DCH, DFFP, MRCGP, General Practitioner
Dr Jonathan Eastwood, BSc, MBChB, MRCGP, General Practitioner
Dr Elizabeth Evans, MA(Cantab), MBBS, DRCOG, Co-founder UKMFA
Dr Christopher Exley, PhD FRSB, retired Professor in Bioinorganic Chemistry
Dr John Flack, BPharm, PhD, retired Director of Safety Evaluation, Beecham Pharmaceuticals, Senior Vice-president for Drug Discovery SmithKline Beecham
Sophie Gidet, RM, Midwife
Dr Ali Haggett, Mental health community work, 3rd sector, former Lecturer in the history of medicine
Dr Keith Johnson, BA, D.Phil (Oxon), IP Consultant for Diagnostic Testing
Dr Rosamond Jones, MBBS, DRCOG, MD, FRCPCH, retired Consultant Paediatrician
Dr Tanya Klymenko, PhD, FHEA, FIBMS, Senior Lecturer in Biomedical Sciences
Dr Caroline Lapworth, General Practitioner
Dr Branko Latinkic, BSc, PhD, Reader in Biosciences
Dr Theresa Lawrie, MBBCh, PhD, Director, Evidence-Based Medicine Consultancy Ltd, Bath
Dr Felicity Lillingstone, IMD, DHS, PhD, ANP, Doctor, Urgent Care, Research Fellow
Dr Geoffrey Maidment, MBBS, DRCOG, MD, FRCP, retired Consultant Physician
Dr Ayiesha Malik, MBChB, General Practitioner
Dr Kulvinder S. Manik, MBChB, MRCGP, MA(Cantab), LLM, Gray’s Inn
Dr Franziska Meuschel, MD, ND, PhD, LFHom, BSEM, Nutritional, Environmental and Integrated Medicine
Dr Graham Milne, MBChB, DRCOG, MRCGP, General Practitioner
Dr David Morris, MBChB, MRCP(UK), General Practitioner
Margaret Moss, MA(Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
Theresa Ann Mounsey, BSc (hons) in midwifery studies
Dr Sarah Myhill, MBBS, Naturopathic Physician, retired General Practitioner
Dr Chris Newton, PhD, Biochemist working in immuno-metabolism














 Bots felled hundreds of jobs at tech giant If time is money, Amazon’s massive internet shutdown Monday cost netizens a pretty penny, as i...
Bots felled hundreds of jobs at tech giant If time is money, Amazon’s massive internet shutdown Monday cost netizens a pretty penny, as i... Emmett Franz: a tale of an Ozarks Bluegrass legend in the making? The Petersens made Emmett Franz and Emmett Franz made the Petersens. T...
Emmett Franz: a tale of an Ozarks Bluegrass legend in the making? The Petersens made Emmett Franz and Emmett Franz made the Petersens. T... From a 2014 report by Paul Conant: The Justice Department severely distorted the evidence it used to pin all blame for the 2001 anthrax ...
From a 2014 report by Paul Conant: The Justice Department severely distorted the evidence it used to pin all blame for the 2001 anthrax ...